
Healthcare in the United States is Pandora’s Box: even the mere thought of it releases physical and emotional curses upon policymakers. We shed some light on one of the aspects of healthcare in the US in our video in Learn Liberty, which is employee benefits and various government policies likening a public option (meaning that creating a government-run health insurance agency that would compete with other private health insurance companies within the United States). In this post, I will address 5 other issues that make healthcare a nightmare in the US–for everyone.
1. Physicians are raising the price of healthcare.
There is a myth that physicians are raising the price of healthcare by adding their “unnecessary” medical malpractice insurance to their patients’ bills. However, that is not exactly correct. Most physicians are only trying to protect themselves from lawsuits that would bankrupt them immediately (most malpractice lawsuits start at $1 million).
For instance, the American Medical Association report showed that 34% of doctors had had a claim filed against them while in practice. The chances of getting sued increase with age. Almost 50% of physicians over the age of 55 have been sued, while about 8% under the age of 40 have been sued. So it is only understandable that they do not want to trash years’ worth of hard work and effort with one lawsuit against them.
There are other unintended consequences of these malpractice claims, too. Most physicians are opting for “defensive medicine” that allows them to cover for themselves. It is the practice of recommending tests or medical treatments that are not necessarily the best option for the patient but mainly serve to protect the physician against the patient as a potential plaintiff. This practice costs about $46 billion a year, according to a 2014 study by Harvard University.
In fact, in most cases, physicians do not even have a lot of control over the prices because there are so many laws governing medicine at the federal and state levels that they mostly have to follow the rules and regulations. For example, within Tampa, costs for the same procedures vary by 1,259%, in Houston, 764%, and in Omaha, 651%.
As for why prices vary so drastically, many hospitals and facilities aren’t upfront with their answers. We know for sure that higher costs of care don’t correlate with better service. In fact, higher costs are often associated with worse experiences with doctors.
2. Insurance companies are raising the price of healthcare.
This is yet another myth that the “greedy” insurance companies are raising premiums and the cost of every treatment for no reason. It is often easy to find one scapegoat for a large problem, and it is almost too easy. The healthcare system in the US is the result of many irresponsible collective decisions made on behalf of the consumers–for years. Starting from the tax-exempt status of healthcare benefits to workers and raising premiums during war times, the US has made many harmful policy changes to the system that left both patients and providers vulnerable.
Insurance companies have risen to the opportunity to externalize these internalities. However, these companies are also heavily regulated and regulated separately in each state. Apart from the increasing costs of being regulated, these companies go through these procedures in every state. “The average American is paying more than $2,000 a year for useless bureaucracy,” said lead author Dr. David Himmelstein, a distinguished professor of public health at the City University of New York at Hunter College in New York City and a lecturer at Harvard Medical School in Boston. Can you imagine the amount of paperwork and administrative labor they drain from the system that could work perfectly fine without any of those?
3. Transparency in Coverage provides consumers with necessary information.
It is an absolute necessity for us, consumers, to know the price of the service we are getting. Price is the number one indicator of the marketplace for both consumers and providers; we know that from Hayek: “In a system in which the knowledge of relevant data is dispersed among millions of agents, prices can act to coordinate the separate actions of different individuals.” Hayek said that in 1979, the US state seems to come to an understanding of this in 2021–only slightly.
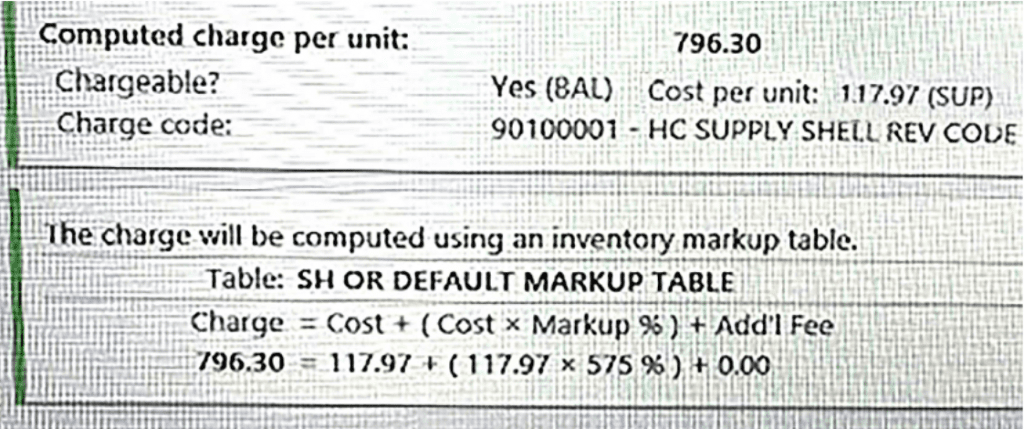
Leaked documents from a hospital in Southern California show that the automatic price markup for these hospitals is 675%. You have read it right: A procedure that costs $117.97 is priced at $796.30. This is just the beginning because this cost does not include extra facility charges such as tests, x-rays, or hospital facilities.
To combat that, states have enacted several laws aimed at improving access to health care price information. Common strategies for improving price transparency include “leveraging all-payer claims databases, establishing consumer-facing tools for patients to compare prices, and enacting right to shop laws.” It has been more than a year since the federal hospital price transparency requirement was announced by the federal government. Currently, 25 states have enacted legislation to implement an APCD system, and 5 states have existing voluntary efforts. According to a July 2022 study by PatientRightsAdvocate.org, only 5.6% of hospitals nationwide are fully following it. Meanwhile, on the other hand, 79% of the voters support the immediate implementation of the federal Transparency in Coverage rule, which requires all healthcare companies to disclose their prices.
4. Obamacare provides everyone with healthcare coverage.
Not correct; there are 7 more federal laws similar to the Affordable Care Act of 2010 (“Obamacare”):
- Medicare
- Medicaid
- Healthcare Quality Improvement Act of 1986 (HCQIA)
- Children’s Health Insurance Program (CHIP)
- Hospital Readmissions Reduction Program (HRRP)
- Health Insurance Portability and Accountability Act (HIPAA) of 1996
- Patient Safety and Quality Improvement Act (PSQIA) of 2005
Each targets a different group of people, developed in a different era, and uses different solutions. Yet one thing connects them all: they all come with very expensive unintended consequences. Obamacare is the last and the most expensive of them.
Essentially, Obamacare relies on three pillars: prevention of insurance companies from denying coverage or raising premiums based on preexisting conditions, requiring everyone to buy insurance, and subsidies to make that insurance affordable. Sounds perfect until it collapses on itself.
If we follow the Obamacare plan, insurance companies must charge the same price to people whether they’re sick or healthy. Many healthy people will view this as a “bad deal” and not buy insurance. This results in higher prices that chase even more people out of the market. It results in a “death spiral” in which only the sick can purchase insurance at very high prices. Obamacare only implements two pillars to…make them disappear to overcome that huge policymaking gap. Everyone should buy it, so there is no “bad deal”, and it should be subsidized to avoid high prices. Take a wild guess at the consequences of this act. Premiums and deductibles have risen to a record-high level while the access and quality of the healthcare services declined as expected. Obamacare might have decreased the number of uninsured individuals, but it did it at the cost of some other individuals.
5. US healthcare is so expensive because there is a huge discrepancy between administrator and physician numbers in the US.
This one is tricky; because it is both correct and incorrect. It is correct that healthcare in the US is insanely expensive, and the system requires more and more administrators every day, which brings the prices up. It is incorrect that there is a large discrepancy, which is why healthcare is so expensive in the US.
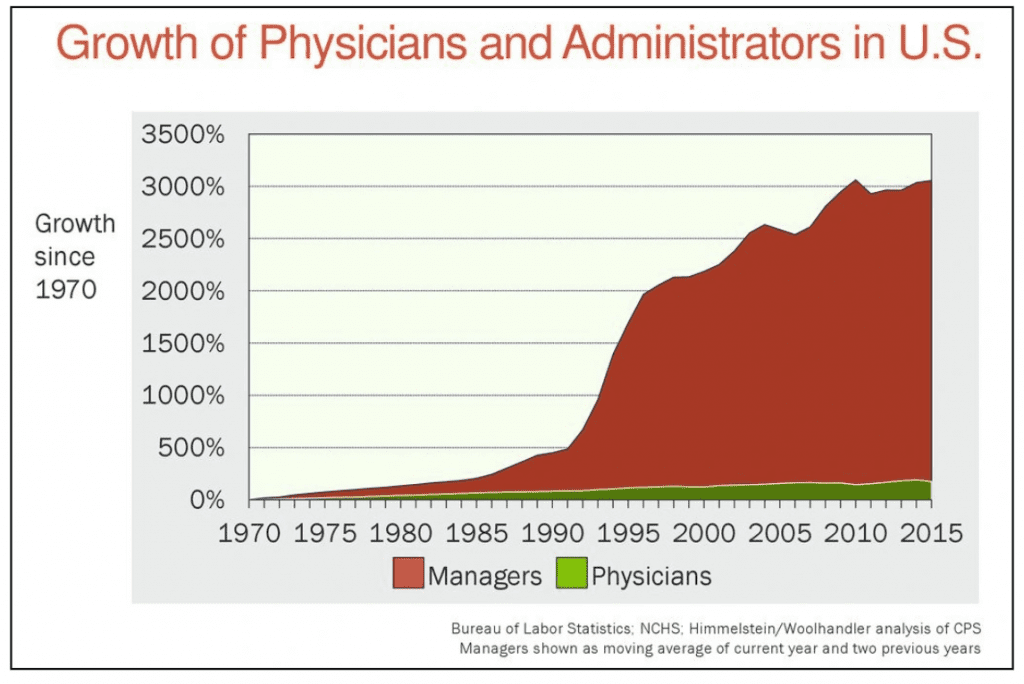
Let’s start with the incorrect part. The famous numbers and the graph below that you probably have seen on social media are misinformation. Healthcare managers have not grown 3000% since the 1970s. There is also no evidence for this graph in the Bureau of Labor Statistics or NCHS whatsoever.
What we have is the numbers from the United States Census Bureau. They suggest that there are roughly 15 million practitioners and medical assistants in the US. We also know that the healthcare industry in the US employs 22 million. This means that there are 7 million non-medical workers in the healthcare industry. Finally, according to the U.S. Department of Labor, the U.S. health insurance industry employed 1 million people in 2020. This means that out of 23 million people in the healthcare industry, 8 million of them have administrative jobs– 34% of the whole industry. That seems reasonable.
One of the shocking things about that graph is the growth rate of practitioners vs. administrators. Since 1970, physicians have only tripled; and administrators have gone from 50,000 to 8 million. That’s a lot! But it’s also not that surprising. In 1970, the healthcare industry spent approximately $0 on IT management. 50 years ago, we didn’t have MRI techs, transplant hospitals, routine ultrasounds for pregnant women, or proton beams for cancer patients. In short, they grew so much because the healthcare industry has grown so much. The US is the leading country in pharmaceutical innovation for a reason. Since 1970, healthcare spending has gone up about 600%, and the number of healthcare workers has gone up about 500%.
However, there is something that we need to mention when it comes to administrative work. Healthcare economists Woolhandler & Himmelstein suggest that “administrative work consumes one-sixth of U.S. physicians’ working hours and lowers their career satisfaction”. Being a physician often means a lot more administrative and legal work than it used to be in the 1970s. Unfortunately, the growing number of administrative staff does not help with that because the bureaucratic burdens are increasing every day. Current trends in U.S. health policy are mostly represented by a shift to employment in large facilities, the implementation of electronic medical records, and the increasing prevalence of financial risk-sharing. These are all likely to increase doctors’ paperwork burdens and decrease their career satisfaction.
RELATED VIDEO:
